

Over 700 health experts are calling for urgent action to expand global production of COVID vaccines
- Written by Deborah Gleeson, Associate Professor in Public Health, La Trobe University
Today, we are joining over 700 health professionals and academics in sending an open letter to Prime Minister Scott Morrison urging him to take a leadership role in expanding the global production of COVID-19 vaccines and other medical tools to fight the pandemic.
The letter, signed by 207 doctors, 177 academics and 111 public health professionals, asks the government to help remove legal and technical barriers to increasing the production of COVID-19 vaccines, diagnostic tests, treatments and other equipment.
We argue there is more Australia — and other wealthy nations — can and should be doing to end the pandemic.
The need to act urgently
The COVID-19 pandemic is escalating sharply in the developing world. In addition to India’s spiralling infections, cases are surging across the globe in countries like Argentina, Uruguay, Sweden, France, Turkey, Mongolia, and Costa Rica.
The roll-out of vaccines must rapidly accelerate. Uncontained transmission will inevitably lead to the emergence of new variants that may be more infectious and resistant to vaccines.
As of today, more than 1.06 billion vaccine doses have been administered worldwide. However, 37% of these doses have been given in the world’s 27 wealthiest countries. Those countries represent just 10.5% of the global population.
Meanwhile, countries making up the least wealthy 11% have received just 1.6% of the vaccine doses so far. At this pace, most of the world’s population will remain unprotected at least until 2023.
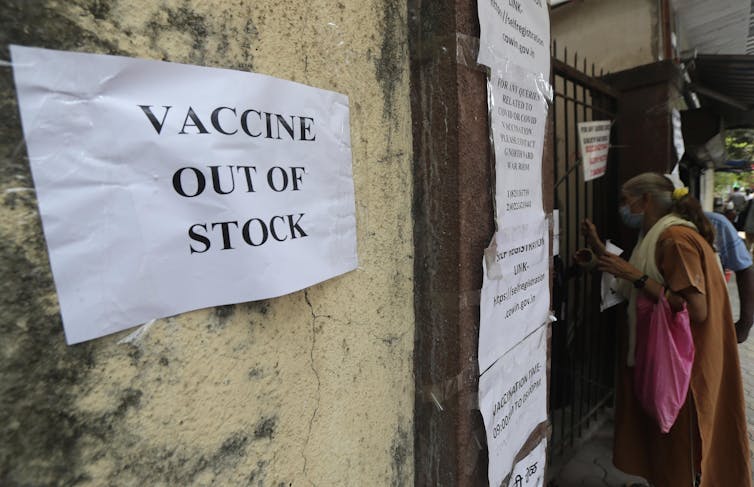 Vaccine shortages have been a frequent occurrence in India in recent weeks.
Rafiq Maqbool/AP
Vaccine shortages have been a frequent occurrence in India in recent weeks.
Rafiq Maqbool/AP
Monopolisation of vaccines
Two of the chief obstacles to vaccinating the world are the monopolisation of vaccines and the means of producing them. The world is relying on the pharmaceutical industry and market forces to solve the problems of inadequate supply and inequitable distribution — and this won’t work.
Rich countries have monopolised the world’s supply of vaccines by pre-purchasing doses in bulk. By November 2020, 7.5 billion doses had been reserved, half of these by rich countries making up only 14% of the global population.
 Countries like Canada have far more vaccines than they need on order.
Paul Chiasson/AP
Countries like Canada have far more vaccines than they need on order.
Paul Chiasson/AP
Rich countries have also under-invested in COVAX, the global program for equitably distributing vaccines. COVAX needs an additional US$3.2 billion just to meet its target of vaccinating 20% of populations of participating countries.
Added to this, countries faced with large outbreaks have erected export restrictions to bolster their own supply of vaccines, excluding others.
This includes the European Union’s refusal to release 3.1 million doses to Australia this year. India has also restricted vaccine exports, resulting in delays in delivering 90 million doses to low-income countries.
The US, too, has been stockpiling its supplies, though the Biden administration announced this week it will now allow the export of raw materials needed to manufacture vaccines in India.
Monopolies on the means of producing vaccines
While the hoarding of vaccines is a concern, the monopolies on the rights to produce them is an even bigger problem.
The exclusive rights to manufacture COVID-19 vaccines are currently held by a small number of companies. These intellectual property rights are enshrined in the World Trade Organization Agreement on Trade-Related Aspects of Intellectual Property Rights, otherwise known as TRIPS.
Under TRIPS, WTO members must allow patents of at least 20 years for new pharmaceutical products, along with other types of intellectual property protection.
Read more: Whoever invents a coronavirus vaccine will control the patent – and, importantly, who gets to use it
TRIPS allows nations to invoke compulsory licensing of pharmaceutical products, which enables patented inventions to be produced without the consent of the patent owner in an emergency.
But compulsory licensing can only be applied on a product-by-product basis, and it only applies to patents, not the other types of knowledge and data needed to manufacture vaccines.
Countries also tend to face diplomatic and trade pressure not to enact such licenses. To our knowledge, no country has yet issued a compulsory licence for a COVID-19 vaccine.
Reliance on the pharmaceutical industry and market forces
So far, the world has placed its trust in the pharmaceutical industry and market forces to solve the problem, hoping vaccine makers would voluntarily enter into licensing arrangements with other manufacturers to increase supply.
But voluntary licensing has been little used to date. When it has been used, it has been done in an ad hoc and opaque way, with restrictive conditions.
AstraZeneca, Gamaleya/Sputnik V and Sinopharm are so far the only companies to implement voluntary licensing for COVID-19 vaccines. AstraZeneca, for instance, has licensed SK Bio in South Korea, the Serum Institute of India and CSL in Australia to manufacture the vaccine.
Read more: The global approach to vaccine equity is failing: additional steps that would help
Other companies’ reluctance to enter into these arrangements means available manufacturing capacity in Asia, Africa, and Latin America is not being used.
The pharmaceutical industry is heavily invested in the status quo. Pfizer and Moderna expect to generate US$15 billion and US$18.4 billion in revenue respectively in 2021, just based on existing supply agreements.
The People’s Vaccine Alliance estimates Pfizer, Johnson & Johnson and AstraZeneca have distributed US$26 billion to their shareholders in the form of dividends and stock buybacks in the past 12 months - enough to cover the cost of vaccinating 1.3 billion people.
 Pfizer/BioNTech’s goal is to produce 2.5 billion doses globally by the end of the year.
Michael Probst/AP
Pfizer/BioNTech’s goal is to produce 2.5 billion doses globally by the end of the year.
Michael Probst/AP
What Australia has done to help so far
Australia has been generous to date, providing AU$80 million to COVAX (specifically for low-income countries).
It has also pledged $523 million to the Regional Vaccine Access and Health Security Initiative, which provides health system support for vaccinations and $100 million to the Quad initiative by India, Japan, Australia and the US, which aims to distribute 1 billion doses in the Indo-Pacific region by 2022.
Australia has also provided 8,840 doses of AstraZeneca vaccine to PNG for frontline health workers and negotiated with the EU to free up 1 million of its own doses on order for PNG. Canberra has also pledged doses to Timor-Leste, Solomon Islands and Vanuatu.
These contributions are important stop-gaps to help address immediate needs. But they won’t go far enough on their own.
 COVID vaccines en route from Australia to PNG last month.
Darren England/AAP
COVID vaccines en route from Australia to PNG last month.
Darren England/AAP
Further steps Australia needs to take
Increasing the global supply of vaccines will require governments to remove legal and technical barriers to their production.
To help remove legal barriers, the Australian government should support a proposal by India and South Africa in October 2020 to waive certain intellectual property rights for COVID-19 medical products.
This proposal, known as the “TRIPS Waiver”, is now supported by more than 100 of the WTO’s 164 member states. However, it has been blocked or stalled by the US, EU, Japan, Canada, and Australia.
Australia will have another chance to support it when it’s discussed at a TRIPS council meeting later this week.
To remove technical barriers, Australia must use its leverage to persuade pharmaceutical companies to share their knowledge and transfer technology to low and middle-income countries.
Australia should also endorse the COVID-19 Technology Access Pool (C-TAP), which was established last May by the World Health Organization but has so far been unused.
C-TAP relies on voluntary commitments by pharmaceutical companies. For it to work, governments need to provide incentives or require pharmaceutical companies to share their IP, data and know-how as a condition of public funding for research and development.
Over 700 health professionals and academics see the government’s leadership in these areas as a critical part of our pandemic response.
It’s time for Australia to act, and to encourage regional allies such as New Zealand, Japan, South Korea, and Singapore to do the same.
Authors: Deborah Gleeson, Associate Professor in Public Health, La Trobe University



